Wishing His Majesty a full and quick recovery
"Wishing His Majesty a full and speedy recovery.
I have no doubt he’ll be back to full strength in no time and I know the whole country will be wishing him well."
Prime Minister Rishi Sunak.
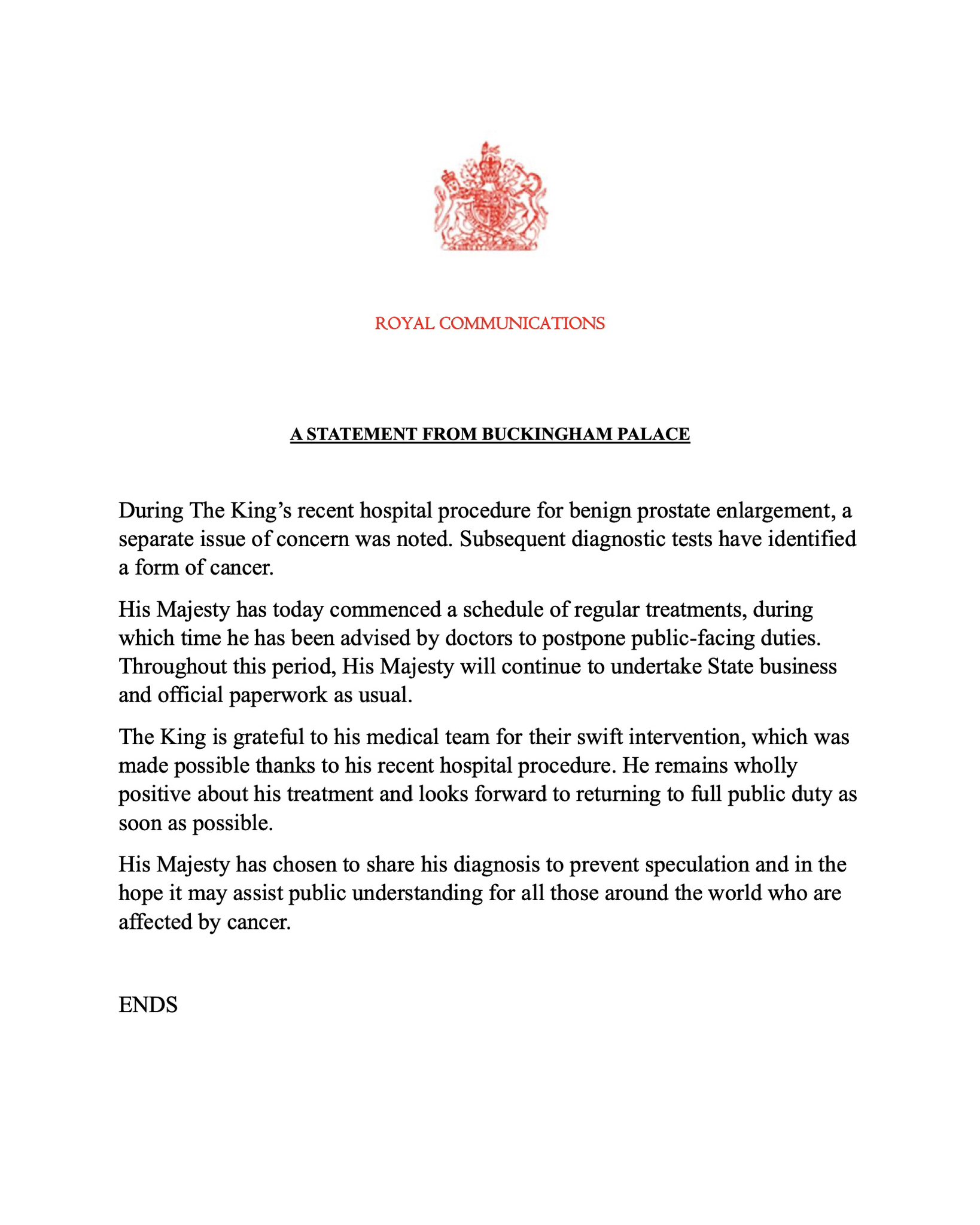
I also, of course, with His Majesty the King a full and speedy recovery following his cancer diagnosis.
For anyone who has not seen it, this was a statement from the palace yesterday:
posted by Chris Whiteside @ 12:34 PM
0 comments
![]()